
Read some patient ambassador experiences below. If you would like your story of how you are involved in patient and public involvement to be added as a blog here, please contact jeanette.boyd@europeanlung.org
Read some patient ambassador experiences below. If you would like your story of how you are involved in patient and public involvement to be added as a blog here, please contact jeanette.boyd@europeanlung.org
Matt Cullen tells about an exciting app which has recently been developed and how he got involved in trying it out
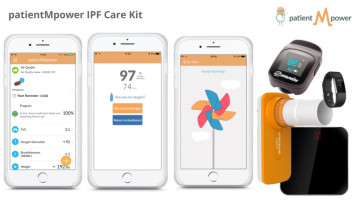
patientMpower, (a company in Dublin, Ireland) have developed an electronic health diary (“an app”) that can be used by people with idiopathic pulmonary fibrosis (IPF) and pulmonary fibrosis (PF) to help them keep a track of their symptoms and lung health.
Colin Edwards and Eamonn Costello from patientMpower came to the Irish Lung Fibrosis Association (ILFA) Dublin Support Group meeting in August 2016 to explain about the app and sought volunteers from the group to try it out and give feedback/suggest improvements on it.
I am a member of the Dublin Support Group and am a patient with IPF (I was diagnosed with idiopathic pulmonary fibrosis in 2010) and I volunteered to try it out along with some other patients in the support group. I agreed to try it out for approximately a month or two and found it so helpful that I have continued to use it ever since.
The app is relatively easy to use and works on any tablet device (such as an iPad) or any Smartphone. For example, the app can be very useful for recording levels of breathlessness, the number of steps walked per day, a reminder to take medicines every day, record oxygen levels and breathing tests results by use of a hand held spirometer.
The spirometer was supplied free of charge from patientMpower and records the FVC (Forced Vital Capacity) by blowing into it and having it close to the Smartphone. The great advantage of recording the FVC on a regular basis is that it can be very useful to obtain objective results over a period of time rather than having to wait maybe six months for a breathing test before seeing a consultant. It also provides an option to record a Journal Entry which can be used for example to record hospital appointments, symptoms such as, rash, nausea as well as diet details and vaccine dates. I found this to be of benefit when attending my respiratory consultant in October 2017 because the information was printed out and I used it to highlight health issues that I was concerned about.
It is worth pointing out, the feedback on the use of the app was very positive from the respiratory clinic, my GP and from other people using that app. PatientMpower deserve credit for actively listening to patients with pulmonary fibrosis, taking patient feedback on board and continuing to improve the app in order to help maximize the benefits to patients using it. Any development of this kind is a very positive step as it helps to empower patients to better manage their health condition.
A pilot study to test the utility and acceptability of an electronic health record (patientMpower) for patients with lung fibrosis was presented at the Connected Health conference in Boston. Another poster entitled: “A longitudinal approach to supported self-management: sustainability of the idiopathic interstitial pneumonia electronic health journal (patientMpower) with integrated home spirometry was presented at the Irish Thoracic Society in Limerick in November 2017.
And hot off the press, news has reached us that patientMpower were one of three winners in the IPF Catalyst Challenge in Chicago awards. Nine finalists pitched their innovative and inspired ideas to help patients living with IPF to a panel of judges. Great news for both patientMpower and very encouraging news for patients that use the App.
Anyone interested in learning more about the app can contact patientMpower at: +353 (0) 1 903 8558, e-mail info@patientmpower.com, also they are on facebook www.facebook.com/patientmpower or visit www.patientmpower.com/ipf.
EPAP patient ambassadors Amanda and Toni (who live in England and Scotland) tell us about their experiences of being involved in the development of clinical guidelines for eczema and asthma
Amanda Roberts: how I got involved in developing NICE Clinical Guidelines: Atopic eczema in children (England, UK)
I have had eczema, hay fever and asthma all my life. It has hospitalised me but I have never allowed it to define me. But it was a different matter when I experienced as a mother the impact of these conditions on loved ones. Both my boys have eczema, hay fever and asthma. My youngest also has anaphylaxis. In particular, because of their eczema, we became frequent visitors to the children’s dermatology out-patient department. One day I noticed a poster saying they were setting up a support group for carers of children with eczema. That was 25 years ago and I am still helping run that group. But now it is web-based and we help people all around the world. We have over 6300 followers on twitter.
Through the group I heard that the National Institute of Health and Care Excellence (NICE) in the UK was going to produce clinical guidelines for the treatment of childhood eczema. Amazingly my application to be on the group that developed these guidelines was successful and I was one of two “patient” voices for that guideline committee. Others on the committee were dermatologists, general practitioners, nurses and pharmacists, all supported by an administrative team. We met one day every month for two years and considered the current evidence for every aspect of management of the condition.
Not only was the guideline supported by a small team of researchers and administrators, but NICE works with what they call “lay people” (patients or carers) on all their guidelines, so there was support for me too. Training at the start, so that I could understand some of the way that they categorised evidence for instance. Media training towards the end of the process when they were looking to publicise the resulting guidelines.
For me, it was inspirational to be with enthusiastic, knowledgeable and caring health care professionals. Frustratingly, not all health care professionals are so interested in eczema. And the guidelines are aspirational not mandatory. From that first work with NICE, and my steep learning curve of technical terms, I have gone on to do other guidelines, research funding panels, standards and even co-applicants in funded health research projects.
Further reading: NICE Clinical Guidelines - Atopic eczema in children (CG57)
Toni-Latimer Simpson: my involvement in the SIGN guideline for Asthma (Scotland, UK)
In 2016 when receiving my usual newsletter from Asthma UK (a national charity), I saw that Healthcare Improvement Scotland were looking for patient advisors to become lay representatives on a Clinical Guideline group looking at the SIGN Guideline for Asthma. SIGN stands for The Scottish Intercollegiate Guidelines Network and they develop and disseminate national clinical guidelines to improve healthcare for patients in Scotland.
Being a patient with asthma myself, I look for new guidance around how to support myself, my family and how to communicate effectively with healthcare professionals when discussing my disease. Also, as I work with healthcare professionals as part of my ‘day job’ in my role as an eLearning Advisor to the School of Pharmacy and Life Sciences at Robert Gordon University in Aberdeen; I felt that it was important that these guidelines had patient input to ensure they are “fit for purpose” for both patients and professionals.
I had a lot of support from Asthma UK who helped me to write the application to become a lay reviewer and I was successfully appointed to the team of lay advisors. Our first task was to transform their patient leaflets for both adults and parents of children with asthma, which accompany the guidelines, into something that was easier to read and understand.
We received training as a group on how to access and read the guidelines as well as on adapting the patient leaflets. We went through the original documents and highlighted any inconsistences and ensured they were user-friendly.
Now, we are in the process of updating the clinical guidelines and this has required us to look at the guidelines to ensure they are up to date and cover what we hope the clinicians should adhere to when discussing asthma with their patients.
We meet again soon in London to discuss our findings and as patients we have been invited to attend to ensure that the patient voice is heard and taken into account.
Overall, my experience has been a good one and I felt the clinicians welcomed our input and insight. Public/patient involvement is a very important part of research and it is hoped that in the future more patients are involved in these areas to bring an important insight in to the guidance of people who actually live with the disease.
Working on the patient information booklets brought me many benefits too, as it meant my name became well known in the asthma community and since I am involved in many other projects, I began to get to know the “usual faces” and to feel more at home.
As with anything that requires input as a patient representative, there can be challenges and I found there were times when I was unable to attend meetings due to my ill-health. Another challenge I faced, is that although my paid employment work is extremely supportive of me taking part in these projects, sometimes I had to ensure that my work took priority.
Overall however, I feel that my impact has been worthwhile. Although the clinicians are subject experts in the field of asthma and lungs, we are expert in being the person living with the condition and sometimes you do have to wonder if they are just favouring us to keep us quiet. I do hope not.
Further reading: SIGN guideline for Asthma (SIGN 153)
My name is Clara Martins de Barros, I live in London, UK, and I am passionate about patient involvement in healthcare. Here I have answered a few questions in an interview with EPAP:
How and why did you become a patient advocate?
I have always wanted to be more proactively involved as a patient advocate, but didn't know how to go about it. It was only when I was a victim of a hate crime a couple of years ago after my move to the UK, followed by a huge disappointing let-down from the counselling services that were meant to be helping with my mental health, and when I started writing to a lot of public and private organisations, that suddenly doors began to open.
I was at rock bottom, and knew that I could only do three things: drown, blame or inspire. So I decided on the latter. As you can imagine, it wasn't that easy or plain sailing. I was alone - I had returned from Portugal after having lived there for a large part of my life - no family or friends nearby, terrified, traumatised, and depressed.
One of the first to contact me was the Institute of Cancer Research (Royal Marsden), where I volunteered in PPI in research, and it was through them that I heard about EPAP. I completed the 7 modules, and then felt better equipped and informed, to start spreading my wings even further.
The significance of this is far deeper than I will ever be able to put into words. It changed my life. It saved my life, really. I will be forever grateful. If you read on, you will see how the learning from those modules is incorporated in everything I do. Since then, EPAP got in touch this year to ask if I would write something for the website.
My life now, little under a year later, consists of having my full time job with my Local Authority and in addition also:
What are the main things you have learnt through your work as a patient advocate?
Medicine isn't just about saving lives, it's about changing lives. Being a patient advocate means utilising the skills I have acquired to help others – to give people hope, to inspire. It means the hard work I put into it, is all worthwhile when health professionals and patients alike, come to me and say 'you have taught me things I have never known before, things that no book, lectures or experience, has taught us. Things that have made me realise that my child is not defective, he/she is just different, and now I know more about his/her inside world'. I speak from the heart and combine my empathy with scientific fact.
What are the main challenges of being a patient advocate?
Being autistic means that I am navigating what is a very hostile/alien environment most days, because of sensory overload. As autistic women in general, we are better at performing normative behaviour, which means I have to use even more of my brain's energy to do this, as normative behaviour isn't something that comes natural to us. To manage my energy levels has been an ongoing big challenge for me – especially as I do all this advocacy work on top of a full time job. I get exhausted.
How have you managed to develop relationships with healthcare professionals?
The best and most effective relationships I have developed with healthcare professionals have been when I let my guard down, or when I reveal who I really am. I tell them that if we value originality, and diversity, we must take risks. Because diversity isn't about being compliant, it's about being different, 'sui generis'. I don't look for acceptance, I look for significance.
I'm not afraid of hierarchy or titles. I also suppose in the Autism world, especially in adult autism, relationships with healthcare professionals are easier, there are fewer barriers – there is generally a huge acceptance that you as the person with Autism are an expert of your Autism. Especially as an adult – you often only get access to diagnosis after self-diagnosis, so the Autism service already knows you are well informed about your condition and up to date research on your condition. They expect it and they are very accepting of this.
As a patient advocate I talk to anyone and everyone. When you want to make a difference in the world, you cannot just be like everyone else, you have to be different. So I am just myself, because I AM naturally different. That's when people stop, look, and listen. The journey continues, but the road is less bumpy now.
We interviewed Daniel Russell, one of our recent patient ambassadors to find out, what got him involved.
How did your involvement as a patient representative begin?
It was towards the end of the year 2012 and I remember my asthma at the time was not very well controlled and I was under the asthma clinic. I was having recurring chest infections which were impacting on my asthma. I had endless test after test, lung function tests, an allergy skin prick test and got seen by various consultants but never fully got to the bottom of it. On one of my visits to the asthma clinic there was a poster on the wall asking for volunteers for the ‘UBIOPRED (Unbiased BIOmarkers in PREDiction of respiratory disease outcomes) study’. I enquired whether I would be able to participate and found out more about the study. Within weeks I was enrolled on the study and I was part of it for a year finding out so much about my asthma, my lung capacity and state of my lungs. First time I had done lung function tests, spirometry, had a CT scan of my chest and bronchoscopy.
What happened after your involvement in the study finished? Did you take part in other projects?
It was on completion of my participation in the study that I was interested in becoming more involved. So, in May 2014 I contacted Asthma UK, my national asthma organisation, about becoming a Research and Policy Volunteer. I quickly became involved in a few research studies, and I gave feedback via email and the internet on some of the studies. This then led on to me joining further PPI (Patient & Public Involvement) groups, one on grant applications and another one at Southampton University Hospital.
How busy has it been for you since then?
Very busy to be honest. Being involved in the different studies and PPI groups led to further involvement, for instance with the Wellcome Trust, and I have applied to be part of myAirCoach, a European research project. There are many more I could mention, but the list would be too long – and all this in only 4 years. I am a patient ambassador with EPAP and also a Patient Research Ambassador with the NIHR in the UK.
What advice would you give patient ambassadors, who would like to get involved in projects, such as you have mentioned?
I think it’s important to be able to influence clinical research, and it’s great that I have the opportunity to do this where I live. You get to interact with senior researchers and clinicians, but most importantly, I feel my views and opinions are both listened to and welcomed by all those involved in PPI. If someone is thinking of getting involved, I’d say “do it”. As well as having a voice and playing a part in the direction of research, you find out so many new things and hear about ideas and studies that could make a huge difference to people’s daily lives and quality of life.

The European Lung Foundation (ELF) organised a patient organisation networking day during the ERS International Congress, the biggest lung congress in the world, which took place in London in September with over 22,000 attending.
Patient organisations have attended this annual congress for many years and this year ELF wanted to give more time to training and networking opportunities for patient organisations. One of the workshops planned for the day was “How EPAP can support your patient organisation”.
After discussing the workshop with the EPAP patient advisory group back in May, two volunteers came forward, happy to help run the workshop - Betty Frankemölle from the Netherlands and Amanda Roberts from the UK.
Both are experienced and very active patient ambassadors, with a history of working for patient organisations in their countries as well as joining international projects.
Click on Amanda and Betty to read their personal experiences of attending this huge congress and what it was like running a workshop for other patient organisations on EPAP.
We also felt that Betty’s and Amanda’s experiences should be passed on to more people and we have therefore decided to incorporate them into the EPAP module “Participating in healthcare conferences”. They will appear there shortly.
If you want to ask Amanda or Betty any questions about their experience, you either email Kerstin Morrison or you can contact them via the comments on the Facebook post relating to this article
This is what we asked some of the patient speakers at the recent ERS International congress. There were 16 patient speakers and demonstrators who participated in the many scientific and educational sessions at the Congress, attended by over 23,000 scientists in an enormous congress centre – a pretty scary thought, even for seasoned speakers. Two patient speakers – Truus Teunissen and Betty Frankemölle from the Netherlands – have agreed to contribute to this article about their experience.
Both Truus and Betty were already interested in patient involvement, either through their work or through their patient organisation. Betty had been asked by Longfonds (the Dutch Lung Foundation) whether she would like to speak at Congress and she was not sure to begin with, as she was worried that her English might not be good enough. Still, having been a volunteer for Longfonds for many years, as well as having been a nurse, Betty decided to take the plunge and give it a go.
All patient speakers were sent an ELF handbook with details of the different sessions, who was who at Congress and practicalities. Truus and some of the other patient speakers had also completed the European Patient Ambassador Programme (EPAP) and especially the new module on “Participating in healthcare conferences”. And yet, there was still a lot of uncertainty of what it would actually be like and what to expect on the day.
Both Betty and Truus liked the fact they were given a guide for the day – this was a healthcare professional, also attending Congress, who contacted them beforehand to introduce themselves, offered help with putting together the slides for their PowerPoint presentations and helped on the day, taking them to their sessions and introducing them to the session chairs (the people who run the session). They found their guides very helpful and reassuring, especially since they were Dutch as well and could help with any language issues.
Truus found the number of people at the congress centre rather intimidating at first and she felt a little insecure speaking in front of a lot of other people in a different language. But she also enjoyed this very much and being able to do this successfully was the highlight of her congress attendance.
Betty sums it up well: “It did very much for my personal development and confidence in myself. Now I know I have to tell something and I am able to tell it.”
My name is Matt Cullen and I am from Dublin, Ireland. I have spent the last 42 years doing voluntary work. From a health perspective the last few years have been difficult, but it has not stopped me doing some voluntary work.
I was diagnosed with idiopathic pulmonary fibrosis (IPF) in 2010 and in 2013 I was diagnosed with chronic obstructive pulmonary disease (COPD) and rheumatoid arthritis (RA). In 2013, it was a particularly difficult time with IPF - I knew no one with this illness at the time, and I consider myself to be very fortunate to have been put in contact with the Irish Lung Fibrosis Association (ILFA) because of the help and support they gave me.
Since then, I have volunteered to help ILFA by taking part in an exercise video (ILFA Exercise DVD for Lung Fibrosis Patients) for patients that have a lung condition. Also, I helped to raise funds for the organisation by donating some of the proceeds from my first solo art exhibition and I act as a contact person for patients that have been diagnosed with IPF to help provide information on the ILFA patient support group, which is held once a month.
It means a lot to me to be of help, even if it appears miniscule compared to the work of others.
Furthermore, I volunteered to take part in a clinical research study which was carried out at Beaumont Hospital, Dublin for patients that have COPD, and I found the EPAP module “Supporting research and development” very appropriate and helpful for this .
I was invited by the European Lung Foundation to speak at the European Respiratory Society Congress in Amsterdam in 2015. The presentation was called: “Why taking the active option is essential for lung health”. To take part in the ERS Congress was a wonderful experience for me. It was great to be able to convey the patient’s perspective to such a wide audience. I was delighted with the help and support from the ELF and the Irish Lung Fibrosis Association. It helped to have completed the EPAP course, especially the module; “Participating in healthcare conferences” as I found it very useful when preparing for the talk and putting the learning into practice.
EPAP has reinforced my belief in the value of patients, irrespective of the condition (or conditions) that they have, all have something worthwhile to contribute. For example, I help out as a patient at times when medical student doctors are doing their final year practical examinations from the Royal College of Surgeons in Ireland. It is great to have patients involved because I believe it helps the medical student doctors to experience patients with rare terminal illnesses such as IPF
Personal health issues in 2016 made it a difficult year for me. This was mainly due to frequent chest infections, an exacerbation of COPD and arthritic problems. However, it had many positives, such as winning Garden of the Year Award in the area where I live, acting as one of the judges in the National Volunteer of the Year Awards in 2016 - I was awarded National Volunteer of the Year Award in 2015. I mention this because such positive experiences help me to keep going. It is interesting to note that some patients with IPF are told that they have about 3 to 5 years to live. I have had IPF for 6 years now. However, I aim to continue to keep active, (such as my active involvement with EPAP) and live life to the full, especially given that I have lived beyond my IPF “expiry” date!

Vanessa Smith, one of our patient ambassadors, recently attended the 1stCOPD Global Patient Leadership Summit. Here are some of her thoughts and experiences of the event.
The 1st COPD Global Patient Leadership Summit, held in Madrid, Spain this month, brought together patients and their representatives from as far afield as Argentina, India, Australia and the UK. Together with physicians, industry partners and health experts, they debated the key issues affecting the worldwide chronic obstructive pulmonary disease (COPD) community. All shared a common goal: to make life better for people who live with COPD in every country of the world.
Patient advocates attending the summit had each completed and submitted a comprehensive pre-summit survey. The results gave a clear picture of the current status of COPD and the challenges faced in their respective countries. Time and again the same core issues were identified, and, whether in Granada or Grimsby, Detroit or Delhi, it was apparent that the time has come for patients to unite, think, and act on a global scale.
Much work was packed into one long day – and a few COPD myths were exploded. One such myth is that COPD is a disease of the elderly – yet, as Monica Fletcher OBE and past chair of the ELF explained, more than half of those diagnosed are in the 40-65 age group.
The stigma surrounding COPD was seen as a major contributing factor to the low priority, low levels of funding and little research it receives. In fact, the term 'stigma' was replaced by 'discrimination' when Dr Inmaculada Alfageme, of the Spanish Society of Pneumology and Thoracic Surgery (SEPAR) spoke passionately and firmly stated, "this is a matter of discrimination – not just stigma – and we have to get past that". This was an issue that every one of us agreed upon.
Other shared experiences included the lack of public awareness, late diagnosis, and the constant references to smoking, reinforcing the widely held perception of COPD as a self-inflicted and deserved condition.
The lack of media attention was discussed. It was noted that barely a day passes without mention of cancer, diabetes, heart disease, etc. yet when journalists or editors asked why they do not produce more COPD articles the responses were that it's not “sexy” or “interesting” and even that "it doesn't affect women”.
The representative from India told us how domestic use of biomass fuel was a major cause of COPD, particularly for the women of his country. With so many living in rural areas, there is often little or no access to medical help. "We have to start from scratch," he said, and no one present was in any doubt as to the size of the task that lay ahead of him.
Despite the challenges, the overall mood was one of determined optimism and camaraderie. COPD is at a tipping point. Governments are starting to realise the cost of ignoring it, and we must capitalise on this – not just as organisations but as individual patients too.
We must galvanise patients from across the world to use social as well as traditional media. We must exert constant pressure on politicians at the local, national and international levels. As John Walsh said, "We may be breathless but we are not without a voice". We intend to use it.

The annual congress of the European Respiratory Society (ERS) is one of the largest and most important in the respiratory calendar. This year it took place in Munich, and was attended by 21,000 delegates! Moreover, thanks to the efforts of Italian lymphangioleiomyomatosis (LAM) patient, Iris Bassi, there were two high-profile LAM events at this year's congress. A morning patient workshop discussed the top priorities of patients living with the disease. Later the same day, a scientific symposium was held at which four leading LAM specialists – including Simon Johnson – presented an update on LAM. For a rare disease such as LAM, it was wonderful to have such well-attended, high-calibre events.
An online questionnaire was distributed widely across Europe and beyond in June/July 2014, which sought to determine the top 10 priorities of women living with LAM. This survey was initiated and coordinated by Iris and staff of ERS's patient arm, the European Lung Foundation (ELF). The results of this survey helped inform the discussions at the patient workshop.
Analysis of the 504 responses identified the following as being the top 10 priorities of LAM patients (in descending order of importance):
The workshop was attended by around 45 people representing patients, patient organisations, medical professionals, researchers and industry from 12 different countries (Austria, Bulgaria, Croatia, France, Germany, Ireland, Italy, Portugal, Spain, Sweden, the US and the UK). Consequently, one of the biggest benefits of the patient workshop was the opportunity for patient representatives and LAM specialists from so many different countries to gather together and exchange ideas.
Clearly, some of the priorities identified in the survey could be acted upon more easily than others. However, this format did provide us with some good topics for small-group discussion. ELF staff led and facilitated the workshop, with a summary of the workshop appearing in the December edition of their publication, Breathe, and the intention to follow up the results of the questionnaire and workshop with an article in a free to access (i.e. open access) academic journal.
In our group, we identified one priority as being particularly important – a possible update to the ERS Guidelines on the Diagnosis, Treatment & Management of LAM. These guidelines are really useful for patients and their doctors, but it is now nearly 5 years since they were published. While much of the information remains the same, experience with sirolimus/rapamycin is now much greater, and the guidelines need to be updated to reflect that experience. Unfortunately, it is not possible simply to add an addendum to the existing ERS guidelines; however, it seems the clinicians discussed this issue after the workshop, and mooted the possibility of joining forces to complete guidelines currently being developed by the Americans. As patients, we should be very supportive of such a move.
One general point raised by many questionnaire respondents was the difficulty in accessing good quality information about LAM, particularly in different languages. Therefore, ERS/ELF has set aside some funding to prepare and publish information about LAM guided by patients, and to be translated into many languages. This is very positive. As yet, I'm not aware of how this would work in practice; it may be difficult to coordinate information amongst so many different organisations. However, a considerable body of information on LAM already exists, and it may be best first to audit what material has already been prepared by national patient organisations and then choose one (or a mixture of more than one) publication to form the basis of that information, which is then translated.
It was a real coup to have four such leading LAM figures – Sergio Harari, Simon Johnson, Joel Moss and Frank McCormack – presenting on the same platform. And that they spoke to a vast auditorium, which was pretty full, is also very encouraging.
Reviewing my notes from the LAM meeting in Barcelona two years ago, it seems that the themes emerging then continue to dominate current thinking:
Thanks are due to Iris Bassi, for her persistence and persuasion, and ERS and ELF for committing time, money and a platform for making these events happen. This was another important step for our rare condition, from which LAM patients will surely benefit.
Why should you consider doing EPAP? Find out what people who have completed the programme thought of it.